NSHN and OSHA Reporting: Prepared to Meet the Deadline?

It is that time of year again. At least for acute care hospitals, long-term acute care (LTAC) hospitals and inpatient rehabilitation facilities (IRF) who report to The National Healthcare Safety Network (NHSN). If annual surveys are not reported by March 1st, then your organization will not be permitted to enter monthly reporting plans until the annual survey has been completed. Although there are just a few weeks to go, early planning is the key.
It is important to consider that responses to the Annual Survey questions are a collaborative effort. Planning a meeting in advance with key stakeholders will help to ease the stress of completing what some may consider to be a daunting task. Be sure to coordinate with Facilities Managers, Pharmacists, Laboratory, Nursing, Infection Prevention and Quality leaders on annual survey responses. Although individuals who are responsible for report submission may find that some of the data has not changed significantly from the previous year, we have identified that some questions have been removed while additional questions have been added.
If you are new to NHSN reporting and have not yet completed an annual survey, you will find an alert reminding you on your dashboard upon logging in. Keep in mind that the survey you are completing requires data from the previous calendar year. You will be submitting data for 2024 due March 1st, 2025. There are a variety of questions that will require information about metrics, facility type, infection prevention practices, laboratory testing methods, water quality management, and antimicrobial stewardship practices for example.
Instructions on completing your organization’s annual survey click on the link below that corresponds with your facility type:
Instructions for Completing Annual Hospital Survey
Instructions for Completing LTAC Annual Survey
Instructions for Completing IRF Annual Survey
OSHA requires the following facilities to complete an annual occupational injury and Illness Report:
- Ambulatory Health Care Servies
- General Medical and Surgical Hospitals
- Psychiatric and Substance Abuse Hospitals
- Specialty Hospitals
- Skilled Nursing Facilities
For a complete list of facilities required to report annually via electronic submission and for additional information on Standard 1904 Subpart E Appendix B click on the following link: OSHA Injury and Illness Reporting Requirements.
Much like NHSN annual surveys, this reporting is also for the prior calendar year. Your deadline for submission is March 2, 2025. If your organization has not previously been reporting, please note that you will need to set up an Injury Tracking Application (ITA) account. For complete instructions, click on the following link User Guide.
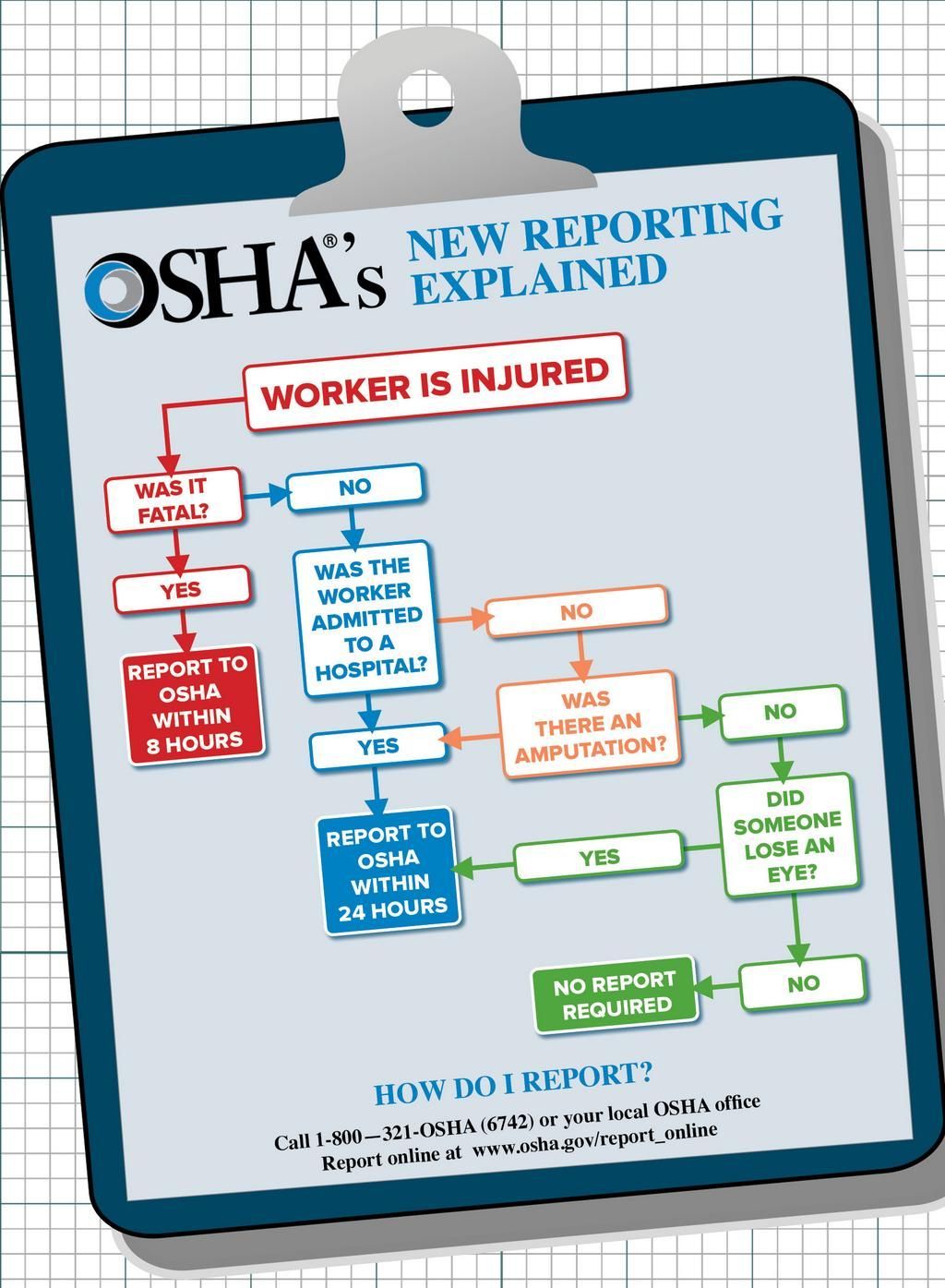
Individuals who are responsible for report completion and submission should have a clear understanding of criteria that constitutes a work-related injury. They will also need to know if the employee missed days of work because of injury or illness. If an employee was restricted from usual work activities or reassigned to a new role as a result of the injury or illness this information must be documented. If an employee required care beyond basic first aid, this will also need to be reported.
Reporters should not include Protected Health Information (PHI). For a brief tutorial on OSHA annual reporting requirements, click on the following link OSHA Injury and Illness Reporting.
Our experts understand the challenges that all healthcare facilities are facing today. Using a customizable approach, we will help you navigate through even the toughest of challenges.
Whether you are in need of mock surveys, leadership training, corrective action plans or ongoing support services, we can help!
We pride ourselves on helping our clients achieve and maintain a status of excellence in the healthcare industry.
Be sure to browse Our Website for a full list of services we provide.
Contact us today at +1 (800) 813-7117 to schedule a free consultation.
References:
https://www.cdc.gov/nhsn/forms/instr/57_103-toi.pd
https://www.osha.gov/laws-regs/regulations/standardnumber/1904/1904SubpartEAppB
https://www.osha.gov/sites/default/files/ita_user_guide.pdf
https://www.osha.gov/sites/default/files/osha_rktutorial.pdf